Introduction
Metal has been used extensively in the manufacturing of orthopedic implants in a multitude of different forms. Multiple different materials throughout history have been tested as replacements for bone. Materials as diverse as ivory, wood, rubber, acrylic, and Bakelite have been used in the manufacture of prosthetic implants.
The extensive use in modern times of metallic alloys is related to the availability and success at the beginning of the 20th century of several different alloys made of the noble metals. Implants made from iron, cobalt, chromium, titanium, and tantalum are commonly used. Clinical studies have demonstrated that alloys made from these metals can be used safely and effectively in the manufacturing of orthopedic implants that are left in vivo for extended periods. The mechanical, biologic, and physical properties of these materials play significant roles in the longevity of these implants.
Implants are made in 3 basic ways:
- Implants can be machine milled or drilled into a desired shape.
- Implants can be cast, which means that the implant is formed from molten metal that is poured into a mold.
- Implants can be forged, which means that the implant is shaped into its final form with the use of forces such as bending or hammering.
Alloys that provide for a long-term stable implant need to have a high level of corrosion resistance as well as certain mechanical properties (see Immune Response to Implants).
Metals
An element is considered metallic if a positive charge is demonstrated on an electrolysis test.1 This test consists of dissolving the element in acid and running a current through the solution. When such elements are fully reduced, their metallic nature is recognized and they and their alloys are called metals; when oxidized, they can serve as ceramic materials.
Metals have several properties that are specific to them, including malleability, which allows the shaping of metal into implants, and ductility, which refers to the ability to draw out metal in the shape of wire and is an important property in allowing the manufacture of intramedullary rods, screws, and long stems. By combining several metallic elements together in alloys, improved properties can be achieved beyond those of a single element. The alloys used in orthopedic surgery need to have certain specific properties. Because the alloy of the implant is bathed in body fluid, a low rate of corrosion and relative inertness are imperative in the material.
All metallic alloys have a modulus of elasticity significantly higher than that of bone. This mechanical incompatibility causes implants to be structurally stiffer than bones. Alloys with elastic moduli closer to bone may cause less stress shielding.
Different metals can form a battery effect when in solution in the body. The galvanic series provides electrochemical comparisons that allow for predictions of corrosion between 2 different metals when they are in physical contact in saline solution.2 Galvanic corrosion occurs if stainless steel surgical wire is wrapped over a cobalt- or titanium-based alloy femoral component or if a cobalt-chromium femoral head is placed on a titanium alloy femoral stem, so this metal mismatch is not recommended. Cobalt- and titanium-based alloy components may be used in contact with each other, and stainless steel components, such as sutures, may be used with either if actual physical contact is avoided.
Surgical Stainless Steel
The introduction of steel plates for fracture treatment is credited to Sherman.3 Surgical stainless steel alloys (316L) made with varying amounts of iron, chromium, and nickel are presently used in the manufacture of prostheses. The low carbon (L) in surgical stainless steel diminishes corrosion and decreases adverse tissue responses and metal allergies. While many implants are still manufactured from this excellent material, its use is relegated mainly to plates, screws, and intramedullary devices that are not meant to be weight bearing for an extended period. Fatigue failure and relatively high corrosion rates make it a poor candidate for the manufacture of modern joint replacement implants.
Chromium-containing iron (and cobalt base) alloys have a chromium oxide–based surface that is a result of passivation or oxidation of the surface. The chromium oxide forms a very thin invisible shield that provides resistance to biodegradation. Because this oxide layer slowly dissolves in vivo, these alloys have a relatively high rate of corrosion. This is evident as a propensity toward both fretting and crevice corrosion, which limits the possibility for biologic fixation or for the manufacture of modular implants.
Cobalt-Based Alloys
Venable and Stuck discovered the battery effects of metals in the body through their testing of the electrolytic effects of various metals on surrounding tissue and bone.1 These tests demonstrated the low level of corrosion of the cobalt-based alloy vitallium. Alloys made of cobalt, chromium, and molybdenum can be used in various different porous forms to allow for biologic fixation by ingrowth. These alloys are among the least ductile when compared to either iron- or titanium-based alloys, making manufacture of these intramedullary rods and spinal instrumentation more difficult. These alloys have some of the highest moduli of elasticity observed in orthopedic implants, and as a result, this was a factor in the stress shielding and thigh pain observed in the first generation of biologically fixed femoral hip implants made with cobalt alloys.4
These alloys are well suited for the production of implants that are designed to replace bone and to be load bearing for an extended period, if not permanently.
The Austin Moore prosthesis and the Thompson prosthesis were manufactured from the cobalt-based alloys. The first-generation biologically fixed implants (ie, porous-coated anatomic [PCA] and anatomic medullary locking [AML] implants) were manufactured of this material. Numerous modern prostheses are still manufactured from this excellent alloy and are used in both cemented and porous forms for hip and knee replacement.
Titanium-Based Alloys
In 1951, Levanthal introduced titanium as a metal for surgery.5 Titanium-based alloys have excellent properties for use in porous forms for biologic fixation of prostheses. The most common is Ti-6 aluminum Ti-4 vanadium (Ti6Al4V), but other more modern alloys are coming into use. Because of the lower moduli of elasticity than cobalt-based alloys or surgical stainless steel, titanium-based alloys have not been found to be as reliable a material when used as a cemented hip replacement. Moreover, its use in total knee replacements has been limited to the nonarticulating parts of the tibial component because of significant wear observed in femoral heads.
Titanium's high level of biocompatibility, low level of corrosion, and modulus of elasticity closer to that of bone allow for its use in numerous porous implants that have yielded excellent long-term results. The low level of corrosion allows for the construction of modular implants that saves in inventory and allows for more precise implant fit.
Current use in various forms is in the production of fracture plates and intramedullary rods and in the production of both femoral and acetabular implants designed for bone ingrowth. Fracture fixation components fabricated from titanium-based alloys are also used preferentially when the implant site is known to be infected or when postoperative shadow-free imaging is desired.
Tantalum and Composites
Tantalum
Tantalum is also remarkably resistant to corrosion and has been used as an ingredient in super alloys, principally in aircraft engines and spacecraft, although 50% of current use is in the form of powder metal for the manufacture of transistors and capacitors. Tantalum can be fabricated in a highly porous form, which has a modulus of elasticity closer to that of bone than stainless steel or the cobalt-based alloys. Tantalum balls have been used in studies that have required bone markers; however, it has not been used in the manufacture of implants until recently. Because of its remarkable resistance to corrosion, tantalum is well suited to a biologic ingrowth setting.
Recent use of tantalum has been in the form of a honeycombed structure that is extremely porous and conducive to bone ingrowth. It is currently available in several forms for bridging bone defects, but its use in the manufacture of femoral stems has yet to occur. Tantalum appears to be a promising metal for use in acetabular reconstruction, but long-term studies need to be conducted.6, 7
Composites
The combination of metallic alloys with other biomaterials can result in implants with improved mechanical and physical properties. Current attempts in designing composite implants have not yielded highly successful results; however, the future possibilities for improvement are promising.
Wear
Different alloys demonstrate different rates of wear. The hardness of an alloy and the smoothness of the bearing surfaces determine its relative rate of wear. Cobalt-chromium-molybdenum alloys and alloys made of stainless steel are more wear resistant than titanium or titanium-based alloys. When breakdown with titanium-based alloys occurs, it is often observed as black areas within the tissues.
Metallic ion release occurs in vivo, and numerous studies demonstrate soluble and precipitated corrosion products, as well as metallic wear debris, in the liver, spleen, lungs, and even remote bone marrow of the iliac crest. The constant motion of the metal-on-metal prosthesis causes a wearing away of the passivated surface and an increase in metallic ion release. The recent interest in metal-on-metal prostheses raises questions of biocompatibility and possible carcinogenic effects that these metallic ions can cause.8, 9, 10
Future Developments
Hopefully, further developments in metallurgy will allow for the development of new alloys that, when compared to current alloys, will have better mechanical and physical properties yielding better long-term results with implants.
The concurrent developments in other biomaterials, such as ceramics, and newer modified polyethylenes, such as cross-linked polyethylene, hopefully will result in improvements in longevity of total joint replacements either with the success of alternative bearing surfaces or with the use of composite materials. The total joint replacement that will last the life of the patient may be a reality one day.11, 12
Multimedia
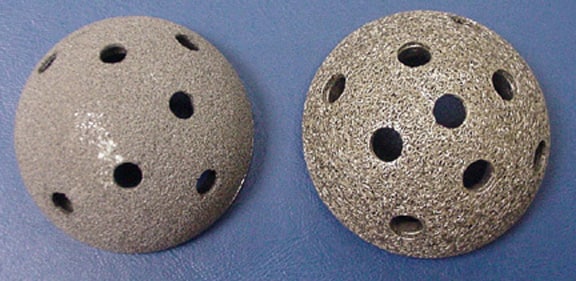
 | Media file 1: Metallic alloys. Tantalum (left) and titanium (right) fiber mesh acetabular cups. |
 | Media file 2: Metallic alloys. Stainless steel Charnley stem (left) and a cobalt-chromium Mueller (right). |

 | Media file 3: Metallic alloys. Composite stems combine the physical properties of alloys with those of other biomaterials. Note, ceramic or metal femoral heads are used on composite hip stems because composites have relatively poor wear properties. |
The shoulder and elbow are comprised of many muscles, ligaments, and tendons that settle the joints, yet they are powerless to harm. Contingent upon how awful the damage is, you may require surgical treatment from an orthopedic specialist who is expertise in Orthopaedic surgery.
ReplyDeleteFor most orthopedic conditions and wounds there might be more than one type of treatment. The Orthopaedic surgeons will talk about treatment choices with the patient to commonly decide thearrangement most appropriate for his/her wellbeing and way of life.
I have being on blog Sites for a while now and today I felt like I should share my story because I was a victim too. I had HIV for 6 years and i never thought I would ever get a cure I had and this made it impossible for me to get married to the man I was supposed to get married to even after 2 years of relationship he broke up with me when he finds out I was HIV positive. So I got to know about Dr. Itua on Blog Site who treated someone and the person shared a story of how she got a cured and let her contact details, I contacted Dr. Itua and he actually confirmed it and I decided to give a try too and use his herbal medicine that was how my burden ended completely. My son will be 2 soon and I am grateful to God and thankful to his medicine too.Dr Itua Can As Well Cure The Following Disease…Alzheimer’s disease,Bechet’s disease,Crohn’s disease,Parkinson's disease,Schizophrenia,Lung Cancer,Breast Cancer,Colo-Rectal Cancer,Blood Cancer,Prostate Cancer,siva.Fatal Familial Insomnia Factor V Leiden Mutation ,Epilepsy Dupuytren's disease,Desmoplastic small-round-cell tumor Diabetes ,Coeliac disease,Creutzfeldt–Jakob disease,Cerebral Amyloid Angiopathy, Ataxia,Arthritis,Amyotrophic Lateral Scoliosis,Fibromyalgia,Fluoroquinolone Toxicity
ReplyDeleteSyndrome Fibrodysplasia Ossificans ProgresSclerosis,Seizures,Alzheimer's disease,Adrenocortical carcinoma.Asthma,Allergic diseases.Hiv_ Aids,Herpe ,Copd,Glaucoma., Cataracts,Macular degeneration,Cardiovascular disease,Lung disease.Enlarged prostate,Osteoporosis.Alzheimer's disease,
Dementia.Lupus.
,Cushing’s disease,Heart failure,Multiple Sclerosis,Hypertension,Colo_Rectal Cancer,Lyme Disease,Blood Cancer,Brain Cancer,Breast Cancer,Lung Cancer,Kidney Cancer, HIV, Herpes,Hepatitis B, Liver Inflammatory,Diabetes,Fibroid, Get Your Ex Back, If you have (A just reach him on drituaherbalcenter@gmail.com Or Whatsapp Number.+2348149277967)He can also advise you on how to handle some marital's issues. He's a good man.
Or Text me on +1-502-2334-479 for more expliant.